Therapeutic Areas
Content is intended for US healthcare professionals only and for educational purposes.
Chronic Rhinosinusitis (CRS)
Chronic rhinosinusitis is a serious nasal inflammatory condition that can significantly harm quality of life and daily functioning. Chronic rhinosinusitis, unlike allergic rhinitis, is characterized by chronic inflammation (not infection, like acute rhinosinusitis) affecting tissues high and deep in the nasal passages, including the area where the openings from the sinuses normally ventilate and drain, causing symptoms that persist for 8 to 12 weeks or longer. Patients with chronic rhinosinusitis may suffer from moderate to severe symptoms for 4 to 6 months a year or more, with symptoms that may be year-round and which often persist for many years.[1]
Chronic rhinosinusitis is defined by 4 diagnostic symptoms[1]:
- Nasal congestion/obstruction
- Facial pain and pressure
- Rhinorrhea (drainage and postnasal drip)
- Loss of sense of smell and taste
Other common symptoms of the condition may include chronically disrupted sleep (often due to difficulty with breathing), headaches, fatigue, halitosis, mood disorders (depression), and other symptoms.[1]
Chronic rhinosinusitis represents an important underserved medical need and a large market opportunity.
- CRS may affect as many as 30 million adults in the United States, half of whom have been diagnosed[2]
- Roughly 7 million people in the United States alone are affected enough that they have undergone nasal/sinus surgery to try to reduce their symptoms, with approximately 600,000 surgeries performed every year[3]
- The US healthcare system has been estimated to spend $60 billion annually in direct costs treating patients with CRS and its associated symptoms[4]
In clinical literature, chronic rhinosinusitis is commonly divided into 2 subgroups: chronic rhinosinusitis with nasal polyps and chronic rhinosinusitis without nasal polyps, however, chronic rhinosinusitis is not an FDA recognized disease indication. For drug development purposes, the FDA has accepted nasal polyps and chronic sinusitis as indications. Nasal polyps are noncancerous growths that arise from inflamed tissue.[1] We estimate that up to 10 million adults in the United States have chronic rhinosinusitis with nasal polyps.[5,6]
Nasal Polyps
Nasal polyps are noncancerous growths that arise from inflamed tissue.[1] Evidence suggests that polyps can also actively promote inflammation, rather than simply resulting from it.[1,6] Up to 10 million adults in the United States have nasal polyps and the associated symptoms (nasal congestion/obstruction, facial pain and pressure, rhinorrhea, and loss of sense of smell and taste).[5,6]
The majority of nasal polyps are located within the ostiomeatal complex and typically originate in the middle meatus around the sinus openings.[7,8] As they grow, polyps mechanically alter and can block the normal flow of air through the nose.[9] Similarly, by blocking the drainage pathways of the paranasal sinuses, sinus inflammation and its associated symptoms occur.[9]
Chronic Sinusitis (CS)
Chronic sinusitis is a common clinical syndrome that affects up to 20 million patients in the United States.[2,5] Chronic sinusitis can be defined as 2 or more of the following symptoms lasting for more than 12 consecutive weeks[10]:
- Nasal congestion/obstruction
- Facial pain and pressureRhinorrhea (drainage and postnasal drip)
- Loss of sense of smell and taste
While healthcare professionals often treat chronic sinusitis with oral and inhaled corticosteroids, nasal saline irrigations, or antibiotics in selected patients,[10] there are currently no approved medications in the United States or Europe for the treatment of chronic sinusitis.
Current Treatments and Limitations
Many patients with chronic rhinosinusitis try multiple treatments to obtain relief, from homeopathic remedies to over-the-counter and prescription medications, often without getting sufficient results. The current therapies to treat chronic rhinosinusitis patients have a number of limitations, including:
- Saline rinses are often recommended and appear to offer some relief, helping to clear particles and debris from areas where normal mucociliary clearance is disrupted by chronic inflammation. They are also time-consuming, sometimes difficult or painful, require water free of pathogens, and are inconvenient.
- Traditional steroid nasal sprays and pressurized aerosols are frequently great for allergies, but unfortunately with chronic rhinosinusitis, they often provide only limited relief
- Oral steroids can be very helpful, but their benefits are short-lived, and even short-term use of oral steroids is associated with significant side effects
- Most other currently available medical management approaches, such as leukotriene inhibitors or long courses of antibiotics, are not well studied and probably have varying degrees of efficacy
- Aspirin desensitization or other immunotherapies may be suitable for certain select patients, as determined by an allergy specialist
- Surgery has been shown to help but is costly, has certain risks, and for a significant percentage of patients does not result in a cure. Ongoing use of medication to control symptoms or even repeat surgery is common
Options for patients who continue to suffer despite trying first-line treatment with regular steroid nasal sprays and saline rinses are limited and potentially costly or higher risk, especially if they prefer not to undergo surgery or have already had surgery.
References
[1] Orlandi RR, Kingdom TT, Hwang PH, et al. International consensus statement on allergy and rhinology: rhinosinusitis. Int Forum Allergy Rhinol. 2016;6(Suppl 1):S22-S209.
[2] Pearlman AN, Chandra RK, Chang D, et al. Relationships between severity of chronic rhinosinusitis and nasal polyposis, asthma, and atopy. Am J Rhinol Allergy. 2009;23(2):145-148.
[3] Bhattacharyya N. Ambulatory sinus and nasal surgery in the United States: Demographics and perioperative outcomes. Laryngoscope. 2010;120(3):635-638.
[4] Caulley L, Thavorn K, Rudmik L, et al. Direct costs of adult chronic rhinosinusitis by using 4 methods of estimation: results of the US Medical Expenditure Panel Survery. J Allergy Clin Immunol. 2015;136(6):1517-1522.
[5] Djupesland PG, Vlckova I, Hewson G. Impact of baseline nasal polyp size and previous surgery on efficacy of fluticasone delivered with a novel device: A subgroup analysis. Am J Rhinol Allergy. 2010;24:291-295.
[6] Hull BP, Chandra RK. Refractory chronic rhinosinusitis with nasal polyposis. Otolaryngol Clin North Am. 2017;50(1):61-81.
[7] Zhong C, Jiang Z, Zhang X. Effect of distribution of nasal polyps in ostiomeatal complex on long-term outcomes after endoscopic surgery. Eur Arch Otorhinolaryngol. 2015;272(12):3757-3762.
[8] Larsen PL, Tos M. Origin of nasal polyps: an endoscopic autopsy study. Laryngoscope. 2004;114(4):710-719.
[9] Becker SS. Surgical management of polyps in the treatment of nasal airway obstruction. Otolaryngol Clin North Am. 2009;42(2):377-385.
[10] Sarber KM, Dion GR, Weitzel EK, McMains KC. Approach chronic sinusitis. South Med J. 2013;106(11):642-648.
For questions, please contact us at medical.services@optinose.com.
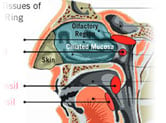
The Anatomy of the Nasal Passages
Experience the anatomy of the nasal passages and how it works.
Exhalation Delivery Systems
See how our products transform nasal treatment.